




Reflecting on APRV-TCAV Outcome Success: Is it the Method or the Manager?
Danielle Hardy, BS, RRT, RRT-ACCS, Adult Respiratory Clinical Specialist, ECU Health Medical Center, Greenville, NC.
Airway pressure release ventilation (APRV) utilizing the time-controlled adaptive ventilation (TCAV) approach is a widely debated subject among respiratory professionals and other clinicians within the critical care community. Medical professionals who disregard this strategy often turn to studies documenting APRV failure. But as described by Andrews, et al., these APRV failure trials did not necessarily follow the guidance of the approach, which may have led to further derecruitment and excessive work of breathing.1 Conducting studies on a nontraditional mode of mechanical ventilation without fully comprehending the method is inappropriate.
Skills require a depth of knowledge
When utilizing APRV-TCAV, issues that arise are not related to the mode of ventilation itself. Instead, they are related to who is managing the ventilator, evaluating the patient thoroughly, and how adjustments are made that lead to success with this strategy. These skills require a depth of knowledge that comes with time and experience. Implementing departmental and health system-wide standardized education on the APRV-TCAV method has tremendously improved the confidence of respiratory therapists in utilizing this strategy in our institution, as well as in the troubleshooting of abnormal ventilator graphics.
As with any other mode of mechanical ventilation, the clinician should be proficient in ventilator waveforms and the interpretation of atypical graphics, along with clinical implications of these gross findings. However, in traditional respiratory programs APRV is only briefly reviewed, as exam-eligible candidates are not tested on nontraditional modes of ventilation.
In the APRV-TCAV method, using a termination of peak expiratory flow rate (T-PEFR) to peak expiratory flow rate (PEFR) ratio of 75% is utilized, as it has been shown to reduce alveolar microstrain and improve alveolar recruitment.2 When using this strategy at the bedside, providers are taught to evaluate and zone in on the value to adjust accordingly to continue to achieve the ratio of 75%.
Many providers are not truly assessing potential issues prior to modifying settings on APRV-TCAV. Providers and clinicians who do not have a solid foundation in troubleshooting abnormal graphics in this method and their associated causes are leading to studies that may have resulted in a misunderstanding of APRV-TCAV. Practitioners should be able to decipher if the patient is showing signs of a restrictive or obstructive process by analyzing waveforms. As clinicians at the bedside, respiratory therapists can interpret waveform graphics and correct the issue appropriately without necessarily adjusting the T-low setting and potentially the pressure high (P-high) setting.
Instructing medical professionals via simulation or real-time education to break down worsened respiratory system compliance into intrapulmonary, extrapulmonary, and mixed classifications has furthered enhanced the understanding of the disease process and expectations of abnormal graphics or changes in monitored values. Reviewing the known causes of issues from increased resistance, whether that be of the circuitry, airway, lungs, or equipment, has improved the knowledge of respiratory therapists and providers at our institution while managing APRV-TCAV.
Standardization is key
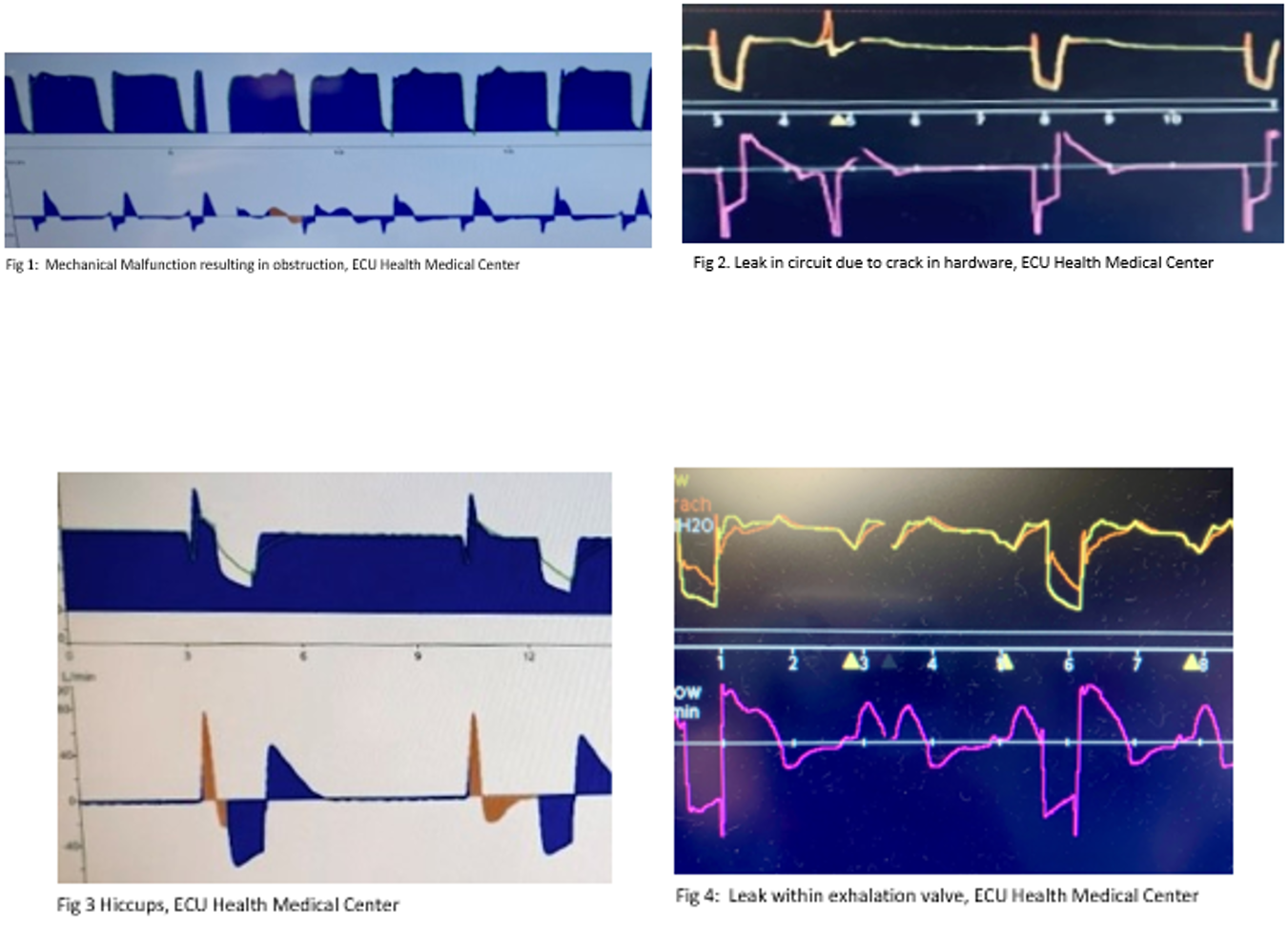
Respiratory therapists could potentially benefit from a standardized approach for education and additional training on recognizing graphic abnormalities that may cause ventilator asynchrony, according to a study conducted by Acho, et al.3 At ECU Health, educational workshops are offered virtually and in a classroom setting. In education and on-boarding training, respiratory therapists learn about the APRV-TCAV strategy with an additional set of clinical skills, such as troubleshooting abnormal waveform graphics in relation to patient assessment (captured in Figures 1-4 here). Understanding how to troubleshoot these findings by capturing examples assisted in our use of the APRV-TCAV method.
During the North Carolina Society for Respiratory Care meeting held September 2022, Dr. Craig Rackley, from Duke Medical Center, and Dr. Hass Al-khalisy, from ECU Health Medical Center, participated in a pro/con APRV lecture.4 Several of the studies debating the con side of APRV were not necessarily completed in the method of the TCAV strategy, nor did they mention troubleshooting ventilator waveforms if issues were to arise.
While researching articles and information regarding troubleshooting the APRV-TCAV method, typically you find papers outlining how to improve oxygenation and assist in ventilation only. It is rare in our profession to discuss patient ventilator asynchrony or the interpretation of abnormal airway graphics using this APRV-TCAV strategy.
If a clinician is not trained in the APRV-TCAV method or on examining the graphics and having a keen understanding of what potentially is causing the issue, then something that could have been fixed with a simple adjustment or intervention such as bronchodilator therapy or even suctioning could cause a larger issue and change outcomes. Respiratory therapists are knowledgeable in waveform analysis and should be able to apply that knowledge to this method of mechanical ventilation.
Seeking more successful outcomes
The APRV-TCAV method is often misunderstood and success relies on the education of the professional managing the ventilator. Respiratory therapists have the capacity to interpret abnormal airway graphics and troubleshoot complications that may arise given respiratory system compliance and resistance. The respiratory profession needs to standardize an educational approach that will result in successful management by providing insight on troubleshooting abnormal graphics and patient-ventilator interaction prior to making modifications to settings.
New graduates are utilizing this strategy in our institution once they have received proper training with the respiratory clinical specialist, re-enforcement by orienting with a skilled preceptor, and have taken courses in regards to this approach. As with any other mode of mechanical ventilation, one must thoroughly assess the patient and graphics prior to making modifications.
As a profession, we need to continue to expand our knowledge, research, and the publication of educational content on APRV-TCAV to include troubleshooting abnormal graphics in different scenarios and strategies that could lead to better and more successful outcomes utilizing this method.5
References
- Andrews P, Shiber J, Madden M, Nieman GF, Camporota L, Habashi NM. Myths and misconceptions of airway pressure release ventilation: Getting past the noise and on to the signal. Front Physiol 2022;Jul 25;13:928562.
- Kollisch-Singule M, Emr B, Smith B, Roy S, Jain S, Satalin J, Snyder K, Andrews P, Habashi N, Bates J, Marx W, Nieman G, Gatto LA. Mechanical breath profile of airway pressure release ventilation: the effect on alveolar recruitment and microstrain in acute lung injury. JAMA Surg 2014;Nov;149(11):1138-45. Erratum in: JAMA Surg 2016;Dec 1;151(12 ):1193.
- Acho M, Kriner E, Sartain NN, Chatterjee S, Sun J, Lee BW, Seam N. Impact of a mechanical ventilation curriculum on respiratory therapist recognition of patient-ventilator asynchrony. Respir Care 2022;67(12):1597-1602.
- Rackley C, Al-khalisy H. Pro/Con APRV. Presented at the 2022 North Carolina Society for Respiratory Care Symposium, Winston-Salem, NC, September 2022.
- Ramirez II, Arellano DH, Adasme RS, Landeros JM, Salinas FA, Vargas AG, Vasquez FJ, Lobos IA, Oyarzun ML, Restrepo RD. Ability of ICU health-care professionals to identify patient-ventilator asynchrony using waveform analysis. Respir Care 2016;62(2):144-149.
HFPV: Lessons Learned in a Burn Center
Elisabeth Caldwell, MBA-HM, RRT, RCP, Director of Clinical Education, St. Philip’s College, San Antonio, TX
Beginning a new role and dedicating time to education has driven me to reflect on how important it is to take opportunities and always add to your repertoire. When I was a new RT, I began working at an adult burn center. As a new graduate, I was exposed to more than I ever imagined. I didn’t realize that my education from traditional respiratory therapy schooling wasn’t where the training stopped. Exposure to new techniques and equipment gave me something invaluable, which is the importance of being a lifelong learner.
At the burn center I worked at, the high frequency percussive ventilator (HFPV) was the ventilator of choice for most of the patients who had sustained inhalation injuries. This may not be common practice at all burn centers, but it was our device of choice for clearing soot and secretions.
Overcoming my fears
It was scary to work with a ventilator I had never used before. Fortunately, thorough training was provided by exceptional therapists who had utilized the ventilator for many years. However, even with hours of training and practice, I still had a fear of making the wrong decisions or picking the wrong settings. But I was determined to never leave the patient worse off than I had received them. I took the leap and decided that I would learn this ventilator and face the challenge head on.
I dedicated myself to learning by spending time after my shift ended trying to manipulate the ventilator to provide the best outcomes for the patients. Senior therapists would drag me out of the room to send me home. But I was determined to be exceptional, and I knew my dedication would pay off.
These skills involved a huge learning curve, and this could have gone wrong. I could have chosen to leave the position and not face the fear of the unknown, or dive into learning. First Lady Abigail Adams is credited with saying, “Learning is not attained by change, it must be sought for with ardor and attended to with diligence.”
I chose to be diligent in my learning.
Surprising outcomes
When we would receive a patient with an inhalation injury, and HFPV was initiated, the outcomes were always surprising. Within days you could see soot and secretions clear from the airway. The ventilator can be used in various ways, where even the smallest changes can improve patient outcomes. Understanding this provides insight that a well-trained therapist, with support of a guiding physician, can use to determine the individual needs of their patient.
Here are some key points that I have encountered through my time spent using HFPV.
HFPV is delivered by a pneumatically powered, flow-regulated, time-cycled, pressure-controlled ventilator.1 Through the use of a sliding venturi, the ventilator delivers sub-tidal breaths to the lungs.
Unlike other high-frequency modes, HFPV does not rely on establishing a higher mean airway pressure to maintain alveolar recruitment. Instead HFPV maintains gas distribution by synergizing with the time constants of the lung compartments, maintaining open alveoli while preventing over inflation.2
By using the smaller, more frequent sub-tidal breaths, they will stack upon each other, allowing for progressively increased lung volumes. Lung volumes are dependent on the patient’s own pulmonary mechanics, but that is where a skilled operator comes in. If a therapist can identify the patient’s needs and observe their status adequately, they have the tools to determine when the patient requires changes.
Clinicians have the ability to change the demand PEEP or the oscillatory PEEP to adjust per patient oxygenation. Pulse frequency can be changed to retain or blow off carbon dioxide.
When comparing the use of the HFPV to the use of a low tidal volume strategy on a conventional ventilator, there was no significant outcome differences noted in one study.3 The real value comes from airway clearance, and particularly in those patients with inhalation injuries.
One outcome noted from the HFPV over the low tidal volume strategy was the low-tidal volume strategy failed to achieve ventilation and oxygenation outcomes, therefore requiring rescue ventilation.3 There might be some insight into how the HFPV is able to clear the airway and assist with secretion management. Humidification is imperative to the outcomes of airway clearance, and maintaining that ideal range is an art form.
Secretion management and humidification are key to success for an inhalation injury. Providing adequate humidification through the HFPV takes a skilled therapist to stay on top of ventilator management for the best patient outcomes. Through the use of continuous nebulization, adequate suctioning, and observation of the airway, inhalation injuries can be improved. These improvements are obtained because the therapist dedicates the time to continuously monitor and assess their patient’s needs.
Building on the foundation
My time in the burn center allowed me to learn new things to build upon my foundational education. Working with the HFPV eventually felt like an art. Manipulating the settings would flow like playing an instrument; sounds even became tools to know if settings were in the right spot.
Taking the leap into a deeper understanding of HFPV paid off and came full circle in the most unexpected way as I was then able to educate others on using the device. I still learn something new every time. I now understand that each patient has individual needs, and their needs can be met in a variety of different ways. Continuing to learn the various ways to treat patients only made me a more diverse therapist.
Using the HFPV was intimidating initially, but taking time to understand the theory behind it gave me insight that is invaluable. As an educator I teach HFPV and other unconventional modalities or treatments to assure others are exposed to new respiratory therapies. As therapists we should strive to remain the go-to person for lung health and continue to advocate for the use of therapies that will benefit our patients.
Now I am the senior therapist, helping nervous new graduates try something new with the added benefit of empathy for their reservations. Every therapist has the ability to keep learning. Understanding advanced modes of ventilation and active engagement in ventilator management with the interdisciplinary team is an important aspect of improved patient outcomes.
My advice is, keep learning. Don’t give up when there is a new obstacle in your way and you will invest in your knowledge, which is irreplaceable.
References
- Kollisch-Singule M, Ramcharran H, Satalin J, Blair S, Andrews P, Habashi NM, Nieman GF, Bougatef A. Mechanical ventilation in pediatric and neonatal patients. Front Physiol 2022;12:805620.
- Lucangelo U, Accardo A, Bernardi A, Ferluga M, Borelli M, Antonaglia V, et al. Gas distribution in a two-compartment model ventilated in high-frequency percussive and pressure-controlled modes. Intensive Care Med 2010;36,2122131.
- Chung KK, Wolf SE, Renz EM, Allan PF, Aden JK, Merrill GA, Shelhamer MC, King BT, White CE, Bell DG, Schwacha MG, Wanek SM, Wade CE, Holcomb JB, Blackbourne LH, Cancio LC. High-frequency percussive ventilation and low tidal volume ventilation in burns: a randomized controlled trial. Crit Care Med 2010;Oct;38(10):1970-1977.
Section Connection
Section discussion list: Go to the Adult Acute Care Section on AARConnect to network with your fellow section members.
Next Bulletin: Please email Karsten Roberts if you would like to contribute an article. He will be happy to help guide you through the process if you’re a new contributor!